Medical rehabilitation as part of ZUS disability prevention is to counteract the threat of partial or total inability to work. Every year the amount of spending on ZUS disability prevention accounts for 0.5% of expenditures for benefits related to inability to work (about PLN 200 million). Medical rehabilitation focused mainly on profiles related to diseases of locomotive organs in stationary and outpatient systems – they made up over 80% of all rehabilitated persons in 2017-2019.
Key audit findings
A medical rehabilitation programme should prevent strengthening organism dysfunctions and thus allow faster return to work. In most cases the key to effective rehabilitation is the short waiting time for its onset. However, in 2017-2019 patients waited for first rehabilitation procedures as long as 110 days on average. In extreme cases it was up to 365 days.
The average waiting time went up in 9 of 11 profiles. For instance, as regards the voice organ, the waiting time increased from 165 to 172 days, for the locomotive system (stationary rehabilitation): from 139 to 142 days, and for the respiratory system from 103 to 122 days. Queuing for rehabilitation went up most in the profile of psychosomatic diseases from 73 to 134 days, for the cardiovascular system in stationary rehabilitation from 83 to 136 days and for the cardiovascular system in outpatient rehabilitation from 59 to 93 days.
According to NIK, such a long waiting time may result in deteriorating health condition of persons who need rehabilitation. Another consequence may be the need to apply additional treatment which may delay the process of restoring ability to work.
The main causes of long rehabilitation waiting time included numerous resignations and failure on part of ZUS to provide a required number of places in rehabilitation facilities.
In 2018-2019, nearly 11.5 thousand and over 10.7 thousand persons respectively resigned from their rehabilitation stay, and almost 9 thousand persons changed the date of the stay in both years. Current legislation does not specify sanctions for unjustified resignation from a rehabilitation stay. ZUS has taken measures to change the law so that the patients who resign from their rehabilitation stays without good reason bear relevant consequences.
ZUS does not have its own rehabilitation centres, so it used facilities owned by the National Health Fund and private rehabilitation facilities. The Social Insurance Institution called for tenders to select them. In 2018-2019, ZUS conducted 67 beauty contests for rehabilitation services as part of disability prevention, of which 11 tenders (16%) were annulled due to the lack of offers and in 18 tenders (27%) only one offer was placed. As a consequence, ZUS could not provide a required number of places in rehabilitation facilities. Key reasons included insufficient number of tenderers meeting the requirements of ZUS and termination of agreements with entities which could not meet contractual terms, especially as regards premises, equipment and medical personnel.
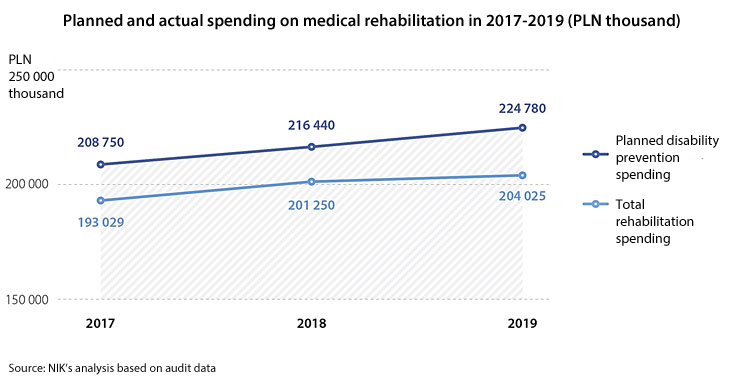
In 2018, it was planned that over PLN 216 million would be spent on medical rehabilitation, whereas in reality a bit over PLN 201 million was actually spent. In 2019, it was over PLN 224 million planned versus PLN 204 million spent. The lower-than-planned spending resulted among others from a smaller number of signed contracts, termination of contracts by rehabilitation facilities and patients’ resignations from rehabilitation stays. The average cost of stay of an insured person in a rehabilitation centre totalled PLN 2.3 thousand in 2019 and was up by 6.4%, compared to 2018.
Most funds were spent on the profile of locomotive organs diseases (in the stationary and outpatient system) and cardiovascular system (stationary rehabilitation). In that period the lowest day rate for rehabilitation stay was PLN 26.54 and the highest day rate was PLN 300.
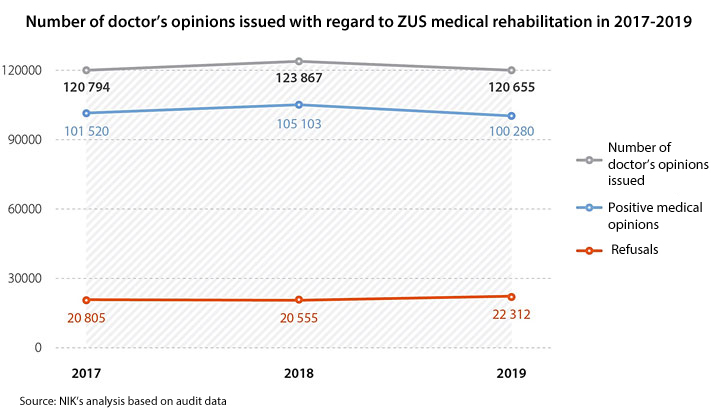
In 2017-2019, the number of doctor’s positive opinions related to medical rehabilitation went down from over 101.5 thousand to nearly 100.3 thousand. In that period, the number of medical opinions saying that rehabilitation is not necessary rose from about 19.8 thousand to nearly 20.4, and the number of rehabilitation refusals for formal reasons went up from over 1.5 thousand to more than 1.9 thousand.
Medical opinions were issued mainly at the request of treating doctors (their number went up from nearly 82 thousand to over 90 thousand), and less and less often by certifying doctors. Reasons included much shorter time for giving opinions and dropping number of requests for benefits.
The key issue for efficient and timely handling of medical opinions is the worsening personnel capacity in ZUS. The audit findings show that the number of certifying doctors and doctors – medical board members is too small for the needs and it is falling every year. ZUS, despite actions taken, has not managed to solve that problem. In 2018-2019, over 13% and nearly 25% of FTEs were not filled out of about 780 and 888 planned FTEs, respectively. NIK has also noted that the average age of certifying doctors and doctors – medical board members exceeded 60 years and in some ZUS branches even 65 years.
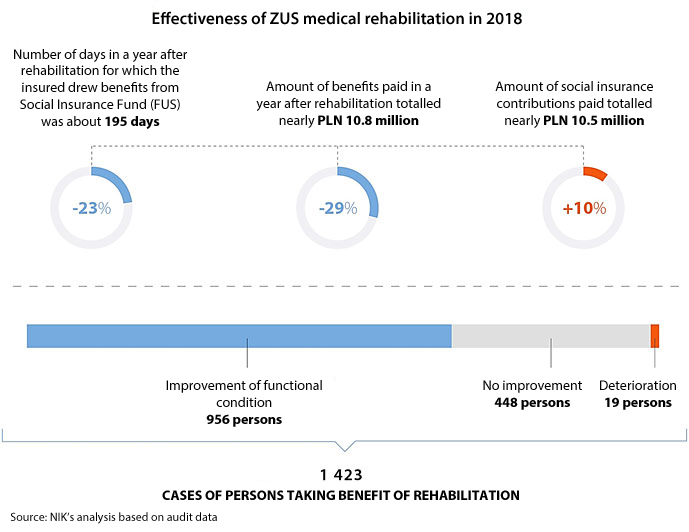
How effective is the medical rehabilitation of ZUS? In the audited sample of 1423 persons, after the end of rehabilitation, the functional condition improved in 956 patients, did not improve in 448 persons and got worse in 19 persons.
According to NIK, effectiveness of medical rehabilitation is falling along with the prolonging period of inability to work of the insured person. The rehabilitation does not fulfil its role in particular with regard to long-term disability pensioners who are low-skilled and out of the labour market or have already got used to the lifestyle ensured by permanent ZUS benefit payment. It is also supported by applicable law, which ensures work to persons drawing disability pensions even if they received medical opinions saying they are totally unable to work.
According to NIK, the method used by ZUS to estimate rehabilitation efficiency is imprecise and so it does not provide reliable data as to the effectiveness of disability prevention.
The effectiveness rate, measured by the failure to draw benefits from the Social Insurance Fund (from Polish: FUS) after one year, was not reliable, because part of those persons did not draw any benefits from FUS before being referred to rehabilitation and a year after its completion. For instance, the persons which drew sickness benefit or rehabilitation benefit for a long time, and then – after completing medical rehabilitation – lost their job or their right to benefits (e.g. the rehabilitation benefit) are considered as effectively rehabilitated persons as they did not draw funds from the Social Insurance Fund. Besides, the effectiveness of medical rehabilitation did not refer to restoring ability to work, which is the primary objective of medical rehabilitation. Besides, when estimating rehabilitation effectiveness the results achieved in rehabilitation facilities were not taken into consideration. Hence, based on the data gathered by ZUS, it is impossible to establish precisely what percentage of people subject to rehabilitation is effectively brought back to the labour market.
Recommendations
to the Minister of Labour to:
- introduce payment obligation or financial liability for persons who resign from rehabilitation without good reason or for persons whose improper behaviour causes shortening of the rehabilitation stay;
- enable ZUS to formulate – in tenders for rehabilitation services as part of disability prevention – tender evaluation criteria other than the price.
to ZUS President:
- take efforts to shorten the average waiting time for medical rehabilitation;
- take efforts to develop adequate indicators to evaluate the medical rehabilitation effectiveness;
- take account of medical rehabilitation results achieved in rehabilitation facilities when evaluating its effectiveness;
- make sure the Information on medical rehabilitation as part of ZUS disability prevention includes evaluation summing up effectiveness of medical rehabilitation in terms of restoring ability to work;
- intensify supervision to reduce significant discrepancies between the description of medical rehabilitation results included in the Information on medical rehabilitation as part of ZUS disability prevention and the actual functional condition of the insured person;
- take actions to identify and eliminate reasons of low effectiveness of medical rehabilitation with persons drawing disability pensions due to temporary inability to work;
- introduce and apply clear principles and criteria of calculating contractual penalties in case rehabilitation facilities fail to comply with contractual terms;
- make inspections in rehabilitation facilities in line with the principles set out in the Rehabilitation management policy;
- address audit recommendations to rehabilitation facilities in line with the principles defined in the Rehabilitation management policy;
- eliminate cases where certifying doctors give their opinions without being properly trained;
- consider introducing the possibility for certifying doctors to refer patients to medical rehabilitation using the so-called „quick path”, in particular in case of persons after medical procedures where immediate rehabilitation is recommended;
- continue efforts to achieve and maintain appropriate employment level of certifying doctors and doctors – medical board members.
